Maxillary rehabilitation after zygomatic implant sequelae using customized subperiosteal implants: a case study
- Apr 28
- 3 min read
Updated: Apr 29
Technological advances in recent decades have further transformed the landscape of Implant Dentistry, introducing tools such as virtual planning, 3D printing, and additive manufacturing. These innovations allow for increasingly precise and individualized solutions, optimizing surgical planning and improving treatment outcomes.
The use of more biocompatible biomaterials and less invasive techniques has expanded the possibilities for successful oral rehabilitation, even in the most challenging cases. Furthermore, new materials beyond the well-established titanium offer new opportunities for aesthetic and functional restorations.
The result of these advancements led to the development of customized subperiosteal implants manufactured through additive manufacturing processes. These implants, particularly indicated for patients with severe bone atrophy, provide effective rehabilitation while avoiding the need for more invasive procedures, such as extensive bone grafts—effectively eliminating the dependence on traditional bone grafting.
CASE REPORT
Female patient with a history of multiple interventions for maxillary rehabilitation. The patient underwent the removal of zygomatic implants and the placement of a customized subperiosteal implant, manufactured through additive processes, in a single surgical procedure.

Initially, the patient was rehabilitated with bilateral zygomatic implants due to severe maxillary bone atrophy. However, chronic inflammation and recurrent infections occurred, leading to implant instability (Figure 2). Given the failure to control the associated peri-implantitis and subsequent complications, the patient was advised to undergo implant removal. Considering the patient's history, treatment with a customized subperiosteal implant was offered.

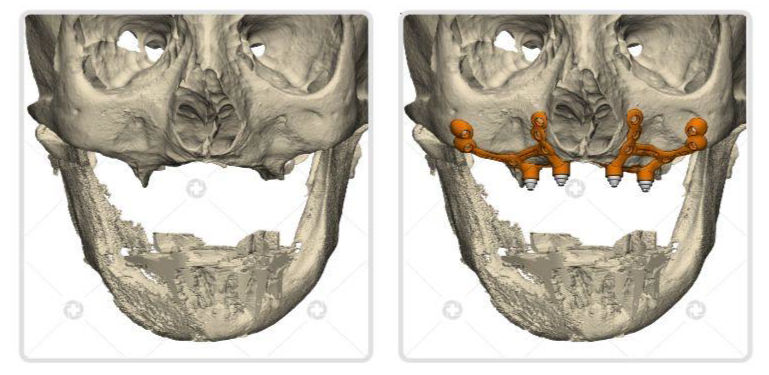
IMPLANT PLANNING
Since this was a customized implant, a computed tomography (CT) scan was sent for virtual planning and simulation for implant sintering according to the manufacturing process. CAD/CAM planning was performed using 3-matic software (Materialise, Leuven, Belgium) (Fig. 3). The implants used were from the CustomLife™ brand (CPMH, Brasília, Brazil).
Once the surgery was scheduled, the implant and prosthetic bar were sintered in Grade 23 titanium (Ti-6Al-4V ELI). Mini-conical abstraction (mini-pillar) prosthetic connections were fabricated. A single-piece implant design was chosen, despite the greater surgical difficulty, due to the potential for higher long-term stability. In addition to the implants and the total prosthesis, the manufacturer provided an osteotomy and drilling guide to ensure implant precision.

SURGICAL PROTOCOL USED
An intraoral vestibular approach was used, with tissue reflection made difficult by previous surgeries. The zygomatic implants, already exposed and lacking bone coverage, were carefully removed using instruments provided by the original surgeon. Following removal, the bone crest was regularized using piezosurgery. Virtual planning guided the osteotomy, smoothing, and creation of support spaces, with the use of guides for greater precision. Subsequently, the customized subperiosteal implant was positioned and fixed to the maxillary bone with titanium screws, ensuring stability and a precise fit, with bone grafting in areas where the zygomatic bone was compromised.

The ability to customize implants to adapt to each patient's unique anatomy offers a viable alternative to traditional approaches, reducing the need for more invasive procedures and improving patients' quality of life. Furthermore, this type of surgery can be considered a rescue option for managing the sequelae resulting from previous dental implant failures.
FINAL RESULT

REFERENCE
CARDOSO, Frederico Rodger Gomes Rodrigues; GRILLO, Ricardo. Maxillary rehabilitation after zygomatic implant sequelae using custom subperiosteal implants: A case study. Journal of Stomatology, Oral and Maxillofacial Surgery, v. 126, n. 5, p. 102154, 2025.

.png)
Comments